

PMS vs. PMDD: Understanding the Difference and What You Can Do About It
The line between difficult PMS and PMDD isn't always obvious, but the difference matters. Here's how to tell, and what to do next.
By Hannah Marsh, Women's Health Guide
Published May 2026 • United Kingdom
Most women are familiar with PMS, the irritability, the bloating, the craving for every carbohydrate in the room. But for some women, what happens in the two weeks before their period is much more than that.
It's the kind of low mood, rage, or hopelessness that genuinely interferes with work, relationships, and daily life. It comes back every single month, like clockwork, then lifts when the period starts.
If that sounds familiar, you're not "just bad at PMS." There's a name for what you're describing, and it's a recognised medical condition with real treatments.
What PMS actually is
Premenstrual syndrome is the cluster of physical and emotional symptoms that show up in the week or two before your period and lift once bleeding begins.
The NHS lists the common ones: mood swings, irritability, low mood, anxiety, tiredness, bloating, breast tenderness, headaches, and changes in appetite or sleep.
It's incredibly common. A systematic review of 17 studies found that around 48% of women experience PMS to some degree. For most, the symptoms are manageable, even if annoying.
Lifestyle changes (regular exercise, less caffeine and alcohol, better sleep, more omega-3s and magnesium) can take the edge off, and many women find their symptoms ease with hormonal contraception.
What PMDD is

Premenstrual dysphoric disorder is, in clinical terms, severe PMS with significant mood symptoms. In practice, it's a different beast.
PMDD affects an estimated 3 to 8% of women of reproductive age, and the symptoms have to be severe enough to interfere with work, school, social life, or relationships. The mood component is the defining feature: deep depression, hopelessness, intense irritability or rage, anxiety that feels overwhelming, and sometimes suicidal thoughts.
These aren't bad-mood-with-a-side-of-bloating. They're symptoms a psychiatrist would recognise as serious, except they show up cyclically and lift within a few days of your period starting.
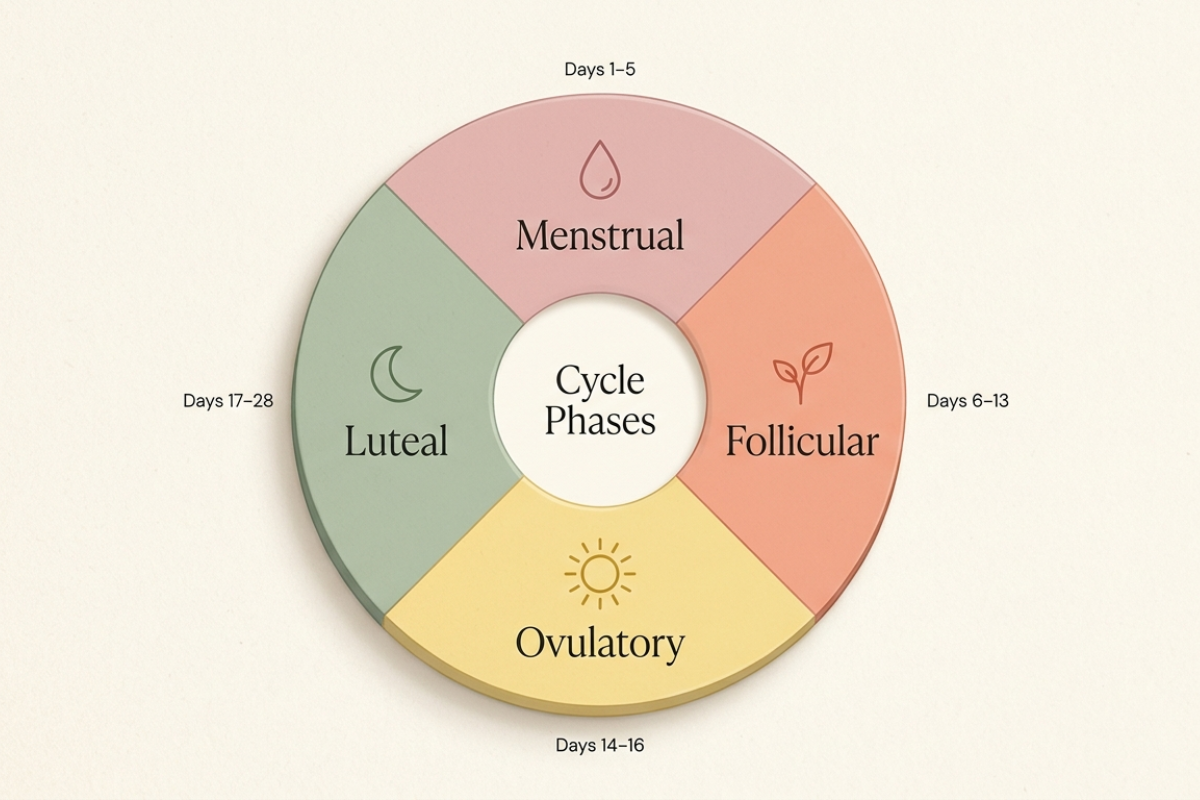
That last detail matters. PMDD is now classified in the DSM-5 as a separate condition under depressive disorders, but unlike depression, the symptoms remit fully during the follicular phase of your cycle (the first two weeks). It's that cyclical pattern that distinguishes it.
PMDD is also linked to significantly higher rates of suicidal ideation, with research showing a four-fold increase in suicidal ideation and a seven-fold increase in suicide attempt risk among women with the condition. This isn't a footnote. It's why getting properly diagnosed and treated genuinely matters.
How they're diagnosed differently
PMS is usually diagnosed based on your description of symptoms and their timing. There's no specific test. Your GP will likely ask about the pattern, severity, and impact on your life.
PMDD has stricter diagnostic criteria. To meet the DSM-5 definition, you need at least five symptoms (with at least one being a mood symptom like depression, anxiety, irritability, or mood swings), occurring in the week before your period for most cycles over the past year, and remitting within a few days of bleeding starting. The catch is that the diagnosis has to be confirmed prospectively, meaning your GP or specialist needs to see at least two months of daily symptom tracking, not just a retrospective description.
This is why symptom tracking matters so much. Without that data, GPs often struggle to distinguish PMDD from depression, anxiety, or other mood conditions, and women can be misdiagnosed or dismissed for years.
What treatments are available for PMDD
There's no single fix, and treatment usually combines several approaches. What works varies hugely from person to person.
Lifestyle changes.
Regular aerobic exercise, reduced caffeine and alcohol, consistent sleep, stress management, and dietary changes (more omega-3s, calcium, magnesium, vitamin B6) have evidence behind them for easing PMDD symptoms. These rarely solve PMDD on their own, but they support other treatments.
Cognitive behavioural therapy (CBT).
There's growing evidence that CBT, particularly tailored to PMDD, can help manage the emotional symptoms and the impact they have on daily life. It's often available through the NHS via talking therapies services.
SSRIs (selective serotonin reuptake inhibitors).
Antidepressants like fluoxetine, sertraline, and citalopram are first-line medical treatment for PMDD. They can be taken continuously or just during the luteal phase (the two weeks before your period). They often work much faster for PMDD than they do for depression, sometimes within days.
Hormonal options.
Combined oral contraceptives (particularly newer ones containing drospirenone) can help by suppressing ovulation. For severe PMDD that doesn't respond to other treatments, a gynaecologist may consider GnRH agonists, which essentially pause the menstrual cycle. Surgery (oophorectomy) is a last resort considered only in very severe cases.
The right approach depends on your symptoms, lifestyle, whether you want hormonal contraception, and your medical history. A GP can start the conversation, but a referral to a gynaecologist or specialist menstrual health service is often helpful.
How to track your symptoms before your appointment

This is the single most useful thing you can do. Free apps (look for ones that specifically support PMDD tracking) work well, or a simple notebook will do. For at least two full cycles, note daily:
Your mood, on a 1 to 10 scale (or more specifically: depression, irritability, anxiety)
Energy levels and sleep quality
Physical symptoms (bloating, headaches, breast tenderness, cramps)
Any impact on work, relationships, or daily functioning
The first day of your period each cycle
After two months, the pattern (if there is one) will usually be obvious: symptoms ramping up in the luteal phase, peaking just before your period, and lifting within a few days of bleeding starting. Bring this to your appointment. It's much harder for a GP to wave you off when you have data.
A word that matters
If you've been told your symptoms are "just PMS" or "all in your head," and you're reading this thinking "but this is destroying my life every month," please believe yourself. PMDD is a real, recognised medical condition. It's not a character flaw, it's not weakness, and it's not something you should have to push through.
The NHS may not have a dedicated PMDD page yet, which makes finding good UK information harder than it should be, but reputable resources do exist (Mind, Rethink Mental Illness, the National Association for Premenstrual Syndromes, and the International Association for Premenstrual Disorders).
You deserve to be taken seriously. Track your symptoms, ask for a referral if you're not getting anywhere, and know that there are people working in this field every day who understand exactly what you're describing.
The bottom line
PMS and PMDD sit on the same spectrum, but they're not the same condition. If your symptoms are mild to moderate and lift quickly, you're probably in PMS territory, and lifestyle changes will usually help.
If your symptoms genuinely disrupt your life, follow a clear monthly pattern, and include serious mood symptoms, it's worth seeing your GP with a symptom diary and asking specifically about PMDD. The diagnosis matters because the treatments are different, and they work.
If you are struggling with thoughts of suicide or self-harm, please contact your GP, call NHS 111, or contact the Samaritans on 116 123 (free, 24/7). You don't have to wait until things get worse to ask for help.
Sources
NHS: Premenstrual syndrome (PMS). https://www.nhs.uk/conditions/pre-menstrual-syndrome/
NCBI / StatPearls: Premenstrual Dysphoric Disorder. https://www.ncbi.nlm.nih.gov/books/NBK532307/
Mind / Rethink Mental Illness: Premenstrual dysphoric disorder (PMDD). https://www.rethink.org/advice-and-information/about-mental-illness/mental-health-conditions/premenstrual-dysphoric-disorder-pmdd/
npj Women's Health: Help-seeking behaviours and experiences for mental health symptoms related to the menstrual cycle: a UK-wide exploratory survey, 2024. https://www.nature.com/articles/s44294-023-00004-w
GPnotebook: Diagnosis of premenstrual dysphoric disorder. https://gpnotebook.com/en-GB/pages/gynaecology/premenstrual-syndrome/diagnosis-of-premenstrual-dysphoric-disorder
London Gynaecology: Premenstrual Dysphoric Disorder (PMDD). https://www.london-gynaecology.com/premenstrual-dysphoric-disorder/
University of Oxford: New data shows prevalence of Premenstrual Dysphoric Disorder (PMDD), 2024. https://www.ox.ac.uk/news/2024-01-29-new-data-shows-prevalence-premenstrual-dysphoric-disorder-pmdd
International Association for Premenstrual Disorders (IAPMD). https://iapmd.org/

You might be interested in




No Commitment, Unsubscribe Anytime
© 2026 Women's Health Guide. All rights reserved